







Join the Leading Global Eye Health Alliance.
Membership-
Choose an alternate language here
- Membership

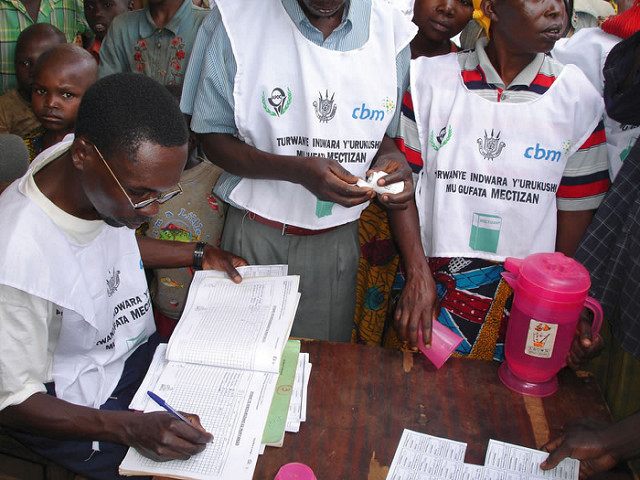
Too many children in Africa go blind due to treatable conditions like cataracts. Child Eye Health Tertiary Facilities (CEHTFs), which typically serve catchment areas of around 10 million people, play a critical role in developing referral pathways and in identifying and managing childhood eye conditions as early as possible to ensure optimal visual outcomes. This requires a multidisciplinary team and strong post-operative follow-up and support systems.
The Kilimanjaro Centre for Community Ophthalmology (KCCO) supports several CEHTFs across Africa, and a key aspect of this support involves training Childhood Blindness and Low Vision Coordinators—a vital cadre in pediatric eye care systems. To scale up capacity building for this essential role, KCCO hosted a regional workshop in July 2025 in Moshi, Tanzania.
The workshop brought together Childhood Blindness and Low Vision Coordinators from Malawi, Uganda, Burundi, Tanzania, the Democratic Republic of Congo, and Madagascar for a week of interactive learning. Participants engaged in expert-led presentations, peer exchange, action planning, and shared reflections on strengthening pediatric eye care in Africa.
Preferred practices for the different roles and responsibilities of the coordinators were discussed. These coordinators bridge clinical, community, and educational systems, with responsibilities that include planning project activities, supporting clinical services, and strengthening referral networks within the health system and through school and community engagement. They train teachers and key informants in early identification, manage follow-ups using tools like SMS reminders, and ensure accurate data collection and reporting.
In child eye health programs supported by KCCO, the involvement of these coordinators has been a key factor in significantly increasing the number of referrals and managed cataract cases—along with other conditions—within the first two years of implementation. Their impact also extends beyond health services to education, rehabilitation, and family support, making them essential to the success of child eye health programs. A summary of key lessons from the workshop will be disseminated in the coming months.
We gratefully acknowledge the support of Seva Canada in making this workshop possible. We also extend our sincere thanks to the Kilimanjaro Christian Medical Centre (KCMC)—a key partner of KCCO—for hosting the workshop and to the KCMC eye specialists who generously contributed their time and expertise by facilitating some of the sessions.









