



Join a powerful, unprecedented alliance for better eye health for all.
Join IAPB-
Choose an alternate language here
Community outreach programmes have been an integral part of Aravind Eye Care System (AECS) from its inception in 1976[i]. For over 4 decades, the outreach eye camps have worked extremely well in identifying and surgically treating cataract patients in high volumes. In the 2018-19 financial year, Aravind Eye Hospitals screened more than 560,000 patients and performed close to 90,000 cataract surgeries through over 2,800 outreach camps[ii].
This approach has significantly contributed in clearing the backlog of cataract blindness, identifying and treating refractive errors and other anterior segment eye problems. However, this model has not been optimal in addressing sight threatening ailments of the posterior segment such as diabetic retinopathy, glaucoma, optic neuropathy, and vascular occlusions.
Conventional Outreach Camps:
In the conventional eye camps, ophthalmologists use torchlight and direct ophthalmoscope for screening while refractionists use streak retinoscope and trial sets for refraction. Intro-ocular pressure is measured using Schiotz tonometer. All the camps use manual paper based medical records. The stations and activities in the camps are well standardised to maximize efficiency and to ensure quality. These camps are designed to provide sustainable eye car to the rural masses by through subsidized prescription spectacles. Cataract surgery including to and fro transport, stay, food and post-operative medications is provided free of cost supported through a subsidy from India’s National Program for Control of Blindness.
Novel Approach to Outreach Camps
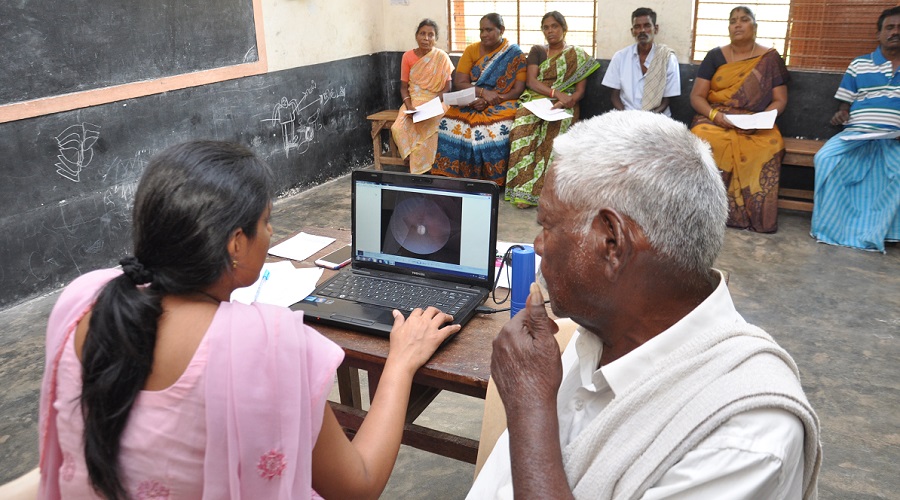
Aravind Eye Hospital Pondicherry, a unit of AECS, has introduced a novel approach to existing outreach with the use of an array of innovative low-cost technology and deploy Electronic Medical Records (EMR). The goal is to enhance the comprehensiveness and yield of eye camps with special focus on posterior segment diseases.
This was initiated in 2017 through a project supported by ‘Seeing is Believing’. This technology intensive model of outreach uses portable and low-cost devices such as i-Care Tonometer (for glaucoma screening), hand-held non-mydriatic fundus camera (for diabetic retinopathy and optic neuropathy), and hand-held slit lamps (for anterior segment disease). These new camps also employs EMR for first time in outreach with laptop and tablet.
The use of technology has led to considerable increase in the rate of early detection of sight threatening problems and referral to the base hospital compared to the conventional approach. The electronic medical record system helps in tracking and following up with the patients referred to the base hospital more effectively compared to the manual paper based medical record system. A comparative analysis of the data showed that the proportion of patients detected in the new approach was around 5% of the total outpatients compared to 1% in the conventional approach. Early detection of the sight-threatening ailments also found to have improved treatment outcomes and reduced treatment costs.
A model for sustainability
Our experience shows that this novel approach of community outreach can address all the broad three aspects of sustainability – Social, Economic and Environmental.
Conclusion:
Community outreach model has already been established as a proven model for mass screening of eye problems in developing countries. Implementing this innovative, low-cost technology oriented approach helps in making outreach camps more comprehensive and effective. Scaling up this model would be beneficial in better coverage of eye care needs in rural populations ensuring all aspects of sustainability.
[i] Natchiar G, Robin AL, Thulasiraj RD, Krishnaswamy S.; Attacking the backlog of India’s curable blind. The Aravind Eye Hospital model; Arch Ophthalmol. 1994 Jul; 112(7):987-93 [PMID: 8031283]
[ii] Aravind Eye Care System-Annual Report 2018-19: https://aravind.org/annual-report/

Authors Name: Vengadesan Natarajan
Author email: [email protected]
Author Job Title: Manager Quality Assurance





















