- A recent systematic review found in India found women have a 35% higher odds of being blind compared to men.3




Join the Leading Global Eye Health Alliance.
MembershipThe recent Lancet commission2 reported:
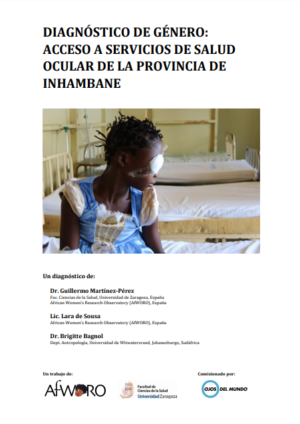
The higher prevalence of vision impairment and blindness in women is attributed to a number of factors, including a longer lifespan, increased risk of developing some eye conditions that can lead to vision impairment and blindness (e.g., age-related macular degeneration, trachomatous trichiasis and cataract) and social inequity contributing to reduced access to care and other inequities.1
The Lancet commission reported on interventions that reduced gender inequity. An intervention included trained rural community volunteers promoting eye services in low- and middle-income countries to women.13 Another intervention examined the effect of free access to cataract testing and low-cost surgery for five years. This intervention reduced the gender disparity in willingness to pay at follow-up five years later.14
The eye health sector has not achieved gender parity, with only 28.3% of eye health organisations boards held by women. Ethnic minority women hold the fewest leadership positions, including the senior management, board position, CEO and chair.15



Jennifer Gersbeck, Gender Equity Working Group Co-Chair and Director of Global Partnerships and Advocacy at the Fred Hollows Foundation, presented as part of an eminent panel which included Dr Jane Goodall and Jessica Smith OAM.

Why the eye health sector must ‘Build Forward Faster’ when it comes to gender and eye health globally.










