







Join the Leading Global Eye Health Alliance.
Membership-
Choose an alternate language here
- Membership
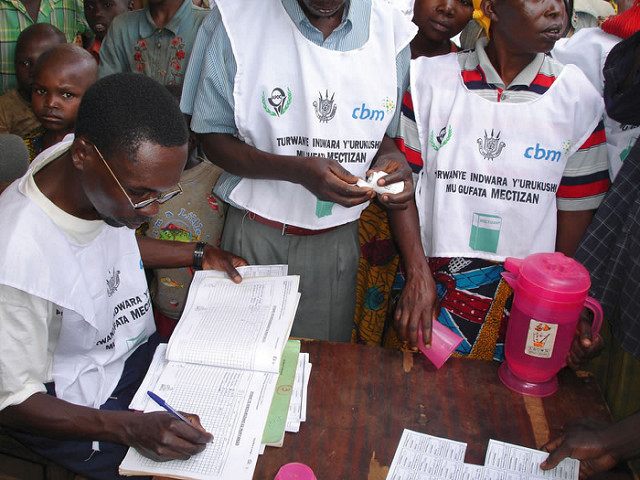
 Trachoma Mapping
Trachoma MappingOphthalmic Epidemiology, 25: Sup. 1
2020 is the target year for the elimination of trachoma as a public health problem.
This issue of Ophthalmic Epidemiology contains a number of articles summarising where the Global Mapping Project has reached, including updates from Ethiopia, Uganda, Congo, Timor-Leste, Nepal, Nigeria, Zambia, Egypt, Senegal, Chad, Yemen, Eritrea, Zimbabwe, Mozambique and Vietnam.
This issue of Ophthalmic Epidemiology contains a number of articles summarising where the Global Mapping Project has reached, including updates from Ethiopia, Uganda, Congo, Timor-Leste, Nepal, Nigeria, Zambia, Egypt, Senegal, Chad, Yemen, Eritrea, Zimbabwe, Mozambique and Vietnam.
Ferriera, G. de A, Rezende, M.A. et al, Barriers between Community Screening for Visual Problems and Treatments in a Tertiary Centre, Rev. Saude Publica, 2018: 52-85
Bangala, C., Gilbert, C., et al: Prevalence, Causes, Magnitude and Risk Factors of Visual Impairment and Blindness in Sri Lanka. Ceylon Medical Journal, 63, 2018
Murthy, G.V. SS, Gilbert C, et al., The Sri Lanka National Blindness, Visual Impairment and Disability Survey: Rational, Objectives and Detailed Methodology, Ceylon Medial Journal, 63, 2018
Ehrlrich, JR., Stagg, B.C., et al: Vision Impairment and Receipt of Eye Care Among Older Adults in Low- and Middle-Income Countries, JAMA Ophthalmology, Nov. 2018 (incudes data from Ghana, South Africa, China, Russia and Mexico)
Radhakrishnan, M., Venkatesh, R., et al: Economic and Social Factors that Influence Households Not Willing to Undergo Cataract Surgery, Indian Journal of Ophthalmology, 63, 2015
Smith, A. F., Negretti G., et al: Glaucoma Control Strategies in Sub Saharan Africa: A Review of the Clinical and Health Economic Evidence, Ophthalmic Epidemiology, July 2018
Elbieh, I, Bascaran, C., et al: Trends in Cataract Surgical Rate and Resource Utilisation in Egypt, Ophthalmic Epidemiology, May, 2018
Winter, G., What Does AI Mean for Optometry, Acuity, Autumn, 2016
Nicole Mohajer & Debra Singh, Factors Enabling Community Health Workers and Volunteers to Overcome Socio-cultural Barriers to Behaviour Change: Meta-synthesis Using the Concept of Social Capital, Human Resources for Health 2018 16:63
Woldie, M., Garumma, Feyissa, T., et al: Community Health Volunteers Could Help Improve Access to and Use of Essential Health Services by Communities in LMICs: An Umbrella Review, Health Policy and Planning, 24 December 2018
Kaunda-Khangamwa, B. N., Steinhardt, L. C., et al: The Effect of Mobile Phone Text Message Reminders on Health Workers Adherence to Case Management Guidelines for Malaria and Other Diseases in Malawi: Lessons from Qualitative Data from a Cluster-randomized Trial, Malaria Journal, 201817:481
Foster, A., A., Makuukula, M., K., et al: Strengthening and Institutionalizing the Leadership and Management Role of Frontline Nurses to Advance Universal Health Coverage in Zambia, Global Health: Science and Practice vol. 6 no. 4 736-746
Badr, E, Mohamed, N.A., et al: Strengthening Human Resources for Health through Information, Coordination and Accountability Mechanisms: The cCase of the Sudan, Bulletin of the World Health Organization 2013;91:868-873.:
Sirili, N., Frumence, G., et al: Doctors Ready to be posted are Jobless on the Street…” The Deployment Process and Shortage of Doctors in Tanzania, Human Resources for Health, February 2019
Sonia and Jeffrey Sachs, Achieving SDG 3. Policy Brief Series 2018
http://unsdsn.org/wp-content/uploads/2018/10/181020-Policy-Brief-Series-5.pdf
The greatest revolution in public health today is the rise of the professionalized Community Health Worker (CHW). CHWs are most effective when professionalized (remunerated, trained, supervised, and provisioned). CHWs are a remarkable bargain, costing $7 annually per person covered. The expansion of CHWs, particularly in low-resource settings, is critical to achieving SDG 3.
“The 2014 Ebola epidemic of West Africa demonstrated the essential role of CHWs. Their relative absence in Liberia, Sierra Leone, and Guinea at the start of the epidemic was one key reason the epidemic spread nearly uncontrolled in the early phase: community health delivery was scant or non-existent in the impacted communities, and communities. …The experience led to a further boost of support by African leaders for CHW deployment. Yet, despite the proven success of CHWs and calls for increased international support for CHW financing, the international community did little at that point to step-up its financing of CHWs….The next breakthrough came with the 2015 decision by Ghana’s former President John Mahama to deploy a national cadre of 20,000 CHWs in Ghana, with a stipend paid by the Youth Employment Agency within the Ministry of Employment and Labour Relations. President Mahama recognized the double benefit of a national CHW program in bolstering public health while providing a valuable career path for young secondary school graduates engaged locally in national service. His successor, President Nana Akufo-Addo, Co-chair of the SDG Advocates, has not only continued the program but is complementing it with a national program of telemedicine for both CHWs and clinics”.
Smith, S. L., Factoring Civil Society Actors into Health Policy Processes in Low- and Middle-income Countries: A Review of Research Articles, Health Policy and Planning, 2019
Jemielniak D, Masukume G, Wilamowski M., The Most Influential Medical Journals According to Wikipedia: Quantitative Analysis, J Med Internet Res 2019;21
Harnessing machine learning to improve health is a major ambition for both medical practitioners and the healthcare industry. If the two can join forces on a global scale in 2019, with the right investment and the right approach, AI [artificial intelligence] could propel a revolution to democratise global health and to leapfrog access to health services in low- and middle-income countries. A chronic shortage of human resources is one of the major obstacles to better health and healthcare in many resource-poor settings. When it comes to global health, artificial intelligence offers huge opportunities to fill the gap left by critical healthcare worker shortages, particularly if combined with mobile phone technology.
For example, social enterprises such as Peek Vision can use smart-phone based technology to enable healthcare providers to deliver cost-effective and targeted treatment to people with eyesight problems. In addition, through developments in personalised care, wearable devices and image recognition for diagnostics, technology is opening up new opportunities for patients to take better care of themselves. With the rise of chronic conditions in nearly all countries, a growing elderly population and stretched health services, empowering patients to help prevent disease makes a lot of sense. With that in mind, public-private partnerships will be strengthened in 2019 to create a suite of robust, effective and equitable digital solutions. These will harness the power of AI to democratise patient power and people’s ability to manage their own health in low and middle-income countries.
Peter Piot is director of the London School of Hygiene & Tropical Medicine and a microbiologist who helped discover the Ebola virus.
(From Nigeria Health Watch, 13/02/19)









