







Join the Leading Global Eye Health Alliance.
Membership-
Choose an alternate language here
- Membership
On World Health Day, Geoffrey Wabulembo, ophthalmologist, CBM writes about his experiences with eye care patients coping with depression.
Pacific Islanders; cropped image from the WHO’s “Depression: Let’s Talk” campaign to mark World Health Day 2017
Kalireku (name changed) worked as an agricultural officer for the civil service. In 2004, he had seen an eye doctor for itchy eyes. He also bought reading glasses from a supermarket when he developed difficulty in reading. In 2014, he presented with loss of vision in the left eye and reduced vision in the right eye. He needed to have his vision restored so he could enjoy his retirement and start a private business as planned. He had already given up driving because of limited vision. After being evaluated he was told that vision could not be restored in the left eye but every effort would be done to preserve what little he had in the right eye.
Diabetic retinopathy had damaged his left eye permanently and severe damage had occurred to the right eye as well. Information about him from other sources indicated that he was very withdrawn. Most likely this was depression and he would have needed support from professional counsellors and possibly psychiatric intervention. Psychiatric referral is usually carried out if the client has severely abnormal behavior and may be dangerous to himself or the society, but where an individual is acting rationally and shows no signs of being aggressive or suicidal, it can be difficult to initiate a discussion on mental health care.
This subject receives little or no attention in most of the plans for eye care and yet on a daily basis we have to deliver bad news to some individuals. The impact of blindness on our patients is mostly observed by the family and yet most of our current interventions occur in the clinic where we examine, counsel, give medications and/or operate on them.
My discussion is not based on systematic follow-up of blind clients with depression but based on observation of different clients and how they struggle to cope with visual loss.
Examples of typical clients:
a. Young clients who have had a catastrophic event: This includes those who previously had good vision and due to, say, a multiple glass injury to their eyes in an accident, eventually lost their sight. They will often consult several clinicians before accepting the fact of irreversible loss of vision. We do not have organised support systems to support them in their depression. Quite often the people around them will consider the depression a normal reaction, expecting that it will go away. Personal communication with an experienced psychiatrist here in Papua New Guinea revealed that she’s not had a direct referral following loss of vision. She however gets several clients seeking mental health services following diagnosis of cancer, HIV and other incurable conditions. Her impression is that families decide that the blind will eventually cope with the new situation.
b. Advanced glaucoma in middle age: These are often patients living a productive life. They are still raising their children. The news of irreversible blindness is often difficult to accept and prompts request for a second opinion and referral to a bigger centre or even abroad. They get depressed but the majority still rely on the family for emotional support. Other patients with progressive retinal and optic nerve diseases, including diabetic retinopathy, who experience prolonged periods of decreasing vision till it gets extinguished, have similar experiences and no systematic mental health support.
c. The cataract patient whose only eye gets complications after surgery resulting in blindness:
The pre-surgical counselling promises restoration of vision. When a complication occurs resulting in vision loss, there is devastation for both the patient and the service provider. Again, without professional mental health support, the client ends up enduring the brunt of the emotional storm.
d. The well informed clients who happen to live in underserved parts of the world:
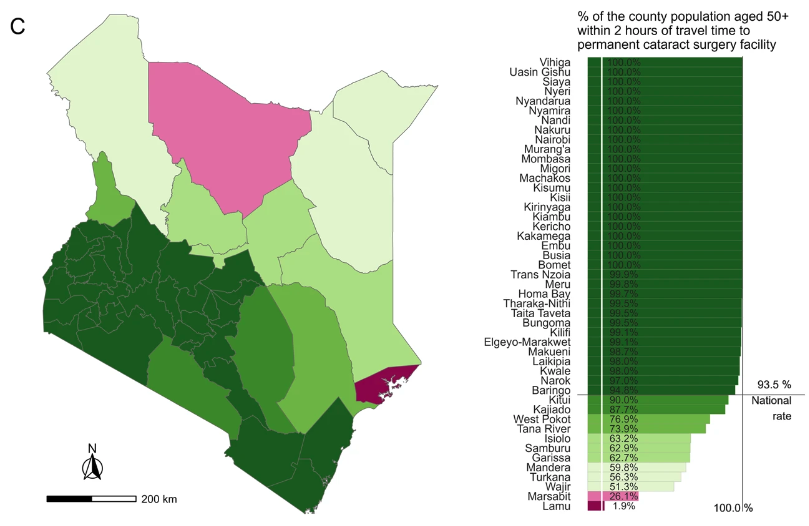
Here I am referring to the many people who have been identified with cataracts but have no access to surgery. They are aware they could have their sight back but have to continue in darkness because they have no access to surgical services. Some have grandchildren they have not seen. This affects their mental health in addition to loss of productivity. Mental health support here could simply take the form of providing the surgical services to restore sight.
For many people the suggestion to see a mental health professional may not be well received, but seeing a counsellor is more acceptable. Having counselling services in the project, but with links to psychiatrists or psychiatric nurses would facilitate access to appropriate services for depression associated with visual impairment. Linking mental health to eye health would benefit many clients whose quality of life tends to be negatively impacted by visual loss. There is a need for deeper understanding of the mental health issues in different cultures associated with severe visual impairment and blindness. We need to provide a system in our eye health plans to address these mental health issues. #LetsTalk #depression #mentalhealth
Liked it? We have more for World Health Day









